
![]()
0 hours
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
0.5 hours
These are activities that require reflection on feedback about your work.
![]()
0 hours
These are activities that use your work data to ensure quality results.
![]()
These are activities that expand general practice knowledge, skills and attitudes, related to your scope of practice.
![]()
These are activities that require reflection on feedback about your work.
![]()
These are activities that use your work data to ensure quality results.

From age 50, the average adult loses 1 to 2% of muscle mass every year—and up to 3% of their strength year on year— says Dr Anita Muñoz, a general practitioner and a medical educator with a special interest in sarcopenia.
These figures escalate dramatically after age 70. “After age 70, leg strength in particular can be lost at rates of 25 to 40% in a decade,” Dr Muñoz says.
Loss of function in the musculoskeletal system can have a devastating impact; it’s associated with higher rates of death and disability, and worsening quality of life. It’s linked with cognitive impairment, metabolic syndrome, depression, difficulty swallowing, falls and fractures and the cascade of effects that follow these, Dr Muñoz explains.
“A decline in our musculoskeletal health causes a decline in everything else,” Dr Muñoz says.
“People die sooner. They survive their medical events for shorter periods of time. They experience poor wound healing. But also their overall chronic disease management is adversely impacted by the loss of their muscle health, strength, and function.”
Yet results from Healthed’s 23 July survey of around 2000 participants found that more than three quarters of GPs do not currently screen for or assess muscle health.
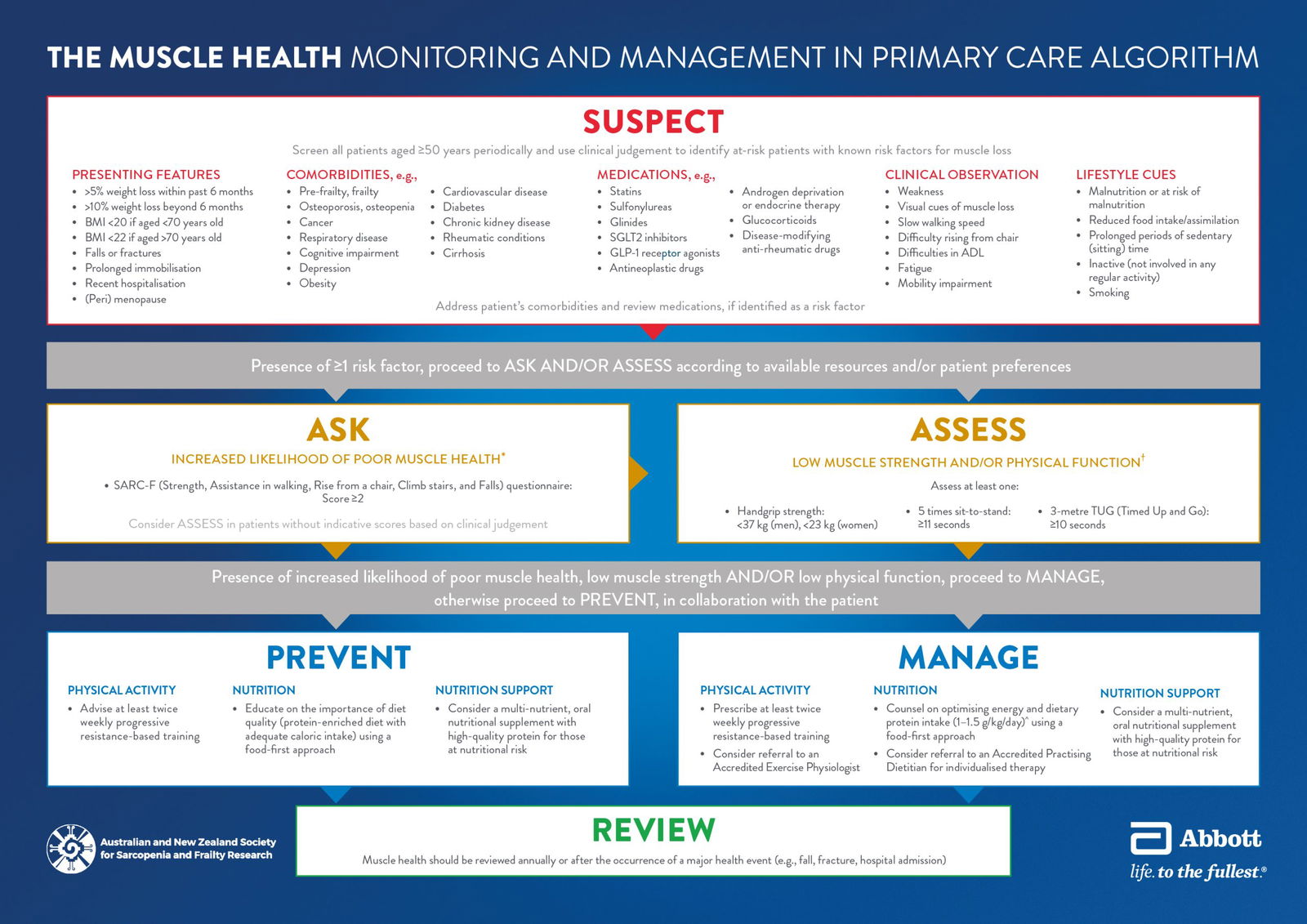
However in May, the Australian and New Zealand Society for Sarcopenia Research and its Expert Advisory Committee* launched an algorithm to help GPs better identify and manage poor muscle health – and prevent sarcopenia where possible.
“This algorithm is designed to detect declining muscle health and not wait until true sarcopenia is present before we intervene,” Dr Muñoz says.
“Knowing that early intervention before muscle mass, strength and function is lost is key, our advisory committee looked at the definitions for sarcopenia in the literature, and recognised that we have an opportunity to take action before those thresholds are met,” she explains.
“We have therefore, applied lower thresholds for defining the need to intervene in preserving muscle health, because acting when sarcopenia has occurred represents a lamentable lost opportunity.”

There are normal declines in muscle, due to the physiological processes associated with ageing, “but there are also superimposed risk factors on top of that that are very important in terms of people’s muscle strength,” Dr Muñoz explains. “So if we have someone who’s got a serious illness, the rate of decline is going to accelerate.”
Being underweight is one of the biggest risk factors for sarcopenia. While overweight or obesity (as measured by BMI) is associated with reduced risk of sarcopenia overall, a 2022 systematic review and meta-analysis found that this was dependent on higher muscle mass and strength. In other words, as this review explains, after adjusting for muscle mass (i.e. the quantity of muscle), higher BMI was actually associated with increased risk of sarcopenia. They note that sarcopenic obesity affects 11% of older adults.
Neurodegenerative disorders such as Parkinson’s disease, certain sleep disorders (short sleep duration and excessive sleep duration), as well chronic conditions, such as diabetes, chronic kidney disease or respiratory disease, and their treatments all negatively impact muscle mass and strength.
Several medications also increase the risk. These are important to consider and review alongside their associated co-morbidities.
Medications that can contribute to poor muscle health include:
Lifestyle factors also play a role.
“A person who is physically inactive has greater than two times the chance of having poor muscle health. And malnutrition has a profound effect on our musculoskeletal system,” Dr Muñoz adds.
“A patient may report to you that they’re not exercising much, they’re not eating well. They may be eating enough calories but not getting enough protein.”
Smoking or drinking excessive amounts of alcohol are also risk factors.
Falls, fractures, illness, and especially recent hospitalisation and ICU stays, also accelerate muscle strength and mass loss.
“Patients who’ve had an episode of acute ill health, particularly needing hospitalisation, or if that person has been in ICU, then those should be cues to us to really think about muscle strength and the need to rehabilitate after really significant medical events have occurred,” Dr Muñoz says.
“When somebody has lost more than 5% of their body weight over six months or more than 10% over a longer period of time, we should assume that some of the muscle mass and strength has been lost in amongst the overall body mass loss,” Dr Muñoz says.
“And of course, we’ve got to have a high index of suspicion for people that are living with multi-morbidity. People with cancer or respiratory illness, metabolic disorders, diabetes, rheumatological disorders are just some of the conditions that impact muscle health.”
If someone appears weak, or you notice their gait is unsteady or not confident, or they have difficulty getting out of a chair, those are also clues that the musculoskeletal system isn’t functioning well.
The algorithm recommends periodically screening all patients from the age of 50, noting that clinical judgement is also important to identify those with known risk factors.
The SARC-F questionnaire is an evidence-based self-reported screening tool that can be used quickly in clinic by either a GP or practice nurse.
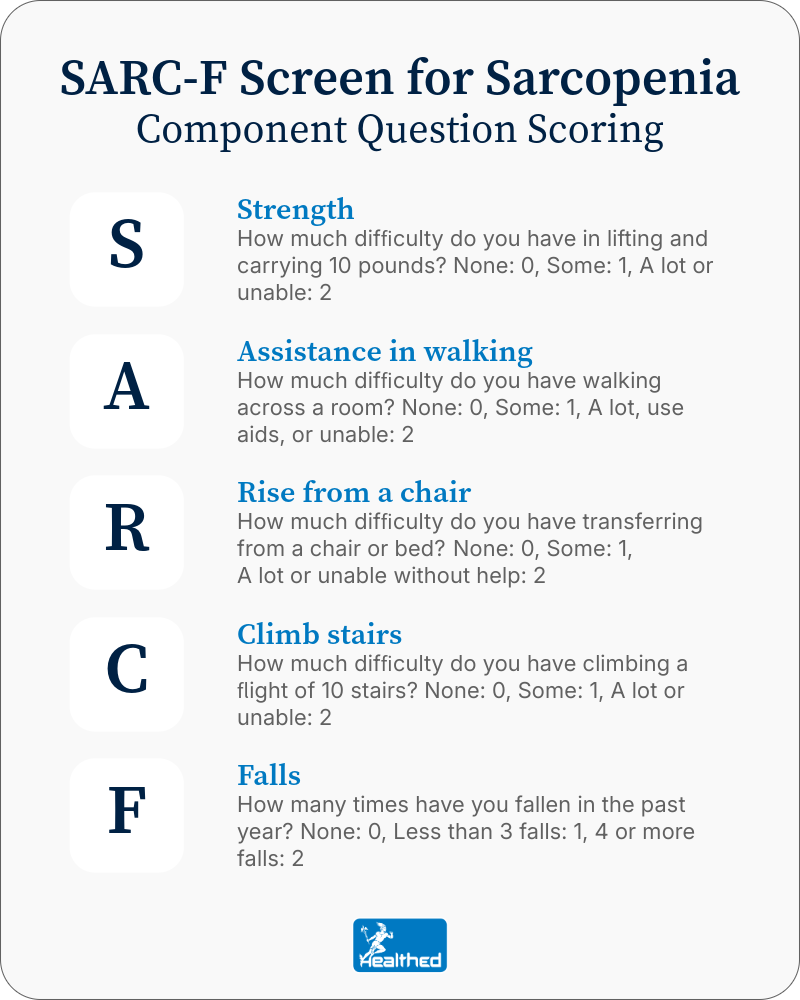
A score of four or more on the SARC-F suggests high risk of sarcopenia, with objective tests of muscle strength (outlined below) needed to confirm this. However, the algorithm has a lower threshold for physical evaluation of muscle strength, recommending it for anyone who reports a score of 2 or more.
“If you’ve got a SARC-F of 2, well then you’ve got a problem with your muscles… if a person’s saying, ‘I’m falling over, I’m struggling to get out of a chair, I’m not confident moving—they’ve got a problem, and they need to have an assessment and a management plan.’”
There are a few reasons to do an objective physical assessment to measure strength. It is a useful benchmark to track progress from the intervention, for one thing. It can also demonstrate “that there is a bona fide problem that needs attention, because some people might need more than just a score from a screening questionnaire to really prove to them that there is an issue with their musculoskeletal health,” Dr Muñoz says.
And if you suspect someone’s muscle health is deteriorating, it can help prove clinical suspicion that isn’t always reflected in SARC-F scores since under-reporting can be an issue, she adds. Muscle strength assessments designed for general practice include:
Dynamometer to assess grip strength
Grip strength is an evidence-based proxy measure of the overall health of the musculoskeletal system.
While the cut-offs for sarcopenia are less than 27 kilos for men or less than16 kilos for women —the algorithm uses less than 37 kilos for a man, or less than 23 kilos for a woman, which already indicates marked decline.
“This algorithm is designed to find poor muscle health and not wait until true sarcopenia is present before we intervene.”
Grip strength can be measured using a hand-held dynamometer. The patient holds the dynamometer at their side with their elbow at a right angle and squeezes as hard as they can with their dominant hand for about 3 seconds. Take the average of 3 attempts.
Sit-to-stand x 5
Using a chair without handles, have the person stand up from a seated position five times.
If a person can’t do this in 11 seconds or fewer, this indicates muscle deterioration that warrants intervention; if they can’t do it in fewer than15 seconds, they meet the criteria for sarcopenia.
Timed up-and-go test
“The person gets up from a chair, walks three meters and back to the chair and sits down.” If it takes longer than 10 seconds, they have lost muscle, while longer than 10.85 seconds indicates sarcopenia.
If you identify poor or declining muscle health, physical activity and nutrition will be key for preventing further deterioration, and ideally, for building strength back up.
At least two days per week of progressive resistance training is recommended, and it’s important that patients are also getting enough protein.
“We need to be recommending at least one, but likely 1.5 grams of protein per kilo per day for our patients to support muscle strength and to support the work they’re doing in their physical strengthening regimens. Now, that’s actually quite a lot of protein. And it’s important to recognise that the dry weight of a food is not necessarily the same as its protein content,” Dr Muñoz says.
“So for example, 100 grams of tuna is not 100 grams of protein.”
She suggests prescribing TGA-approved protein supplements for those struggling to meet the requirements.
Collaborative teams are also crucial, and should include both an exercise physiologist and a dietitian, she says.
When to review
Even if someone’s muscle strength is good, it’s important to provide prevention advice and review every one or two years, since ageing itself increases the risk of decline.
“We recommend reviewing muscle health when a new diagnosis is made or when new medications are prescribed to a patient, particularly those conditions in the ‘suspect’ section of the algorithm,” Dr Muñoz says. Those include pre-frailty/frailty, osteoporosis/osteopenia, cancer, respiratory disease, cognitive impairment, depression, obesity, cardiovascular disease, diabetes, chronic kidney disease, rheumatic conditions and cirrhosis.
“I use time, new medical diagnoses or medications, and hospital stay as important prompts to review a person’s musculoskeletal health.”
Based on this educational activity, complete these learning modules to gain additional CPD.




Browse the latest articles from Healthed.















