

In recent speeches to the AMA last month and to internal staff and board members a few weeks before that, AHPRA CEO Justin Untersteiner said he was not convinced that the current notifications system has what it takes to instil trust.
That would require a system that is timely and efficient, demonstrates high levels of procedural fairness, is transparent with strong and clear communication, and is empathetic and accessible, he said.
“I am not convinced that the current notifications end-to-end system is achieving those important qualities, and as a result it is leading to a loss of confidence and a loss of trust in the scheme,” Mr Untersteiner said.
“We need to pick the whole system up and rethink it,” Mr Untersteiner said.
The tone of Mr Untersteiner’s speeches stood out to some AHPRA-watchers, but will we see real improvements to the way complaints are handled?
Nearly one in two GPs don’t think so, a Healthed survey of more than 1600 GPs has found.
The 48% who think change is unlikely cited a myriad of reasons. Many GPs were sceptical about the ability to change a deeply entrenched culture and ensconced bureaucracy. Several felt the organisation was “too set in their ways,” with people resistant to change, and lacking understanding of clinicians’ perspectives. Others noted AHPRA’s past failures to implement changes and a history of promises without follow through.
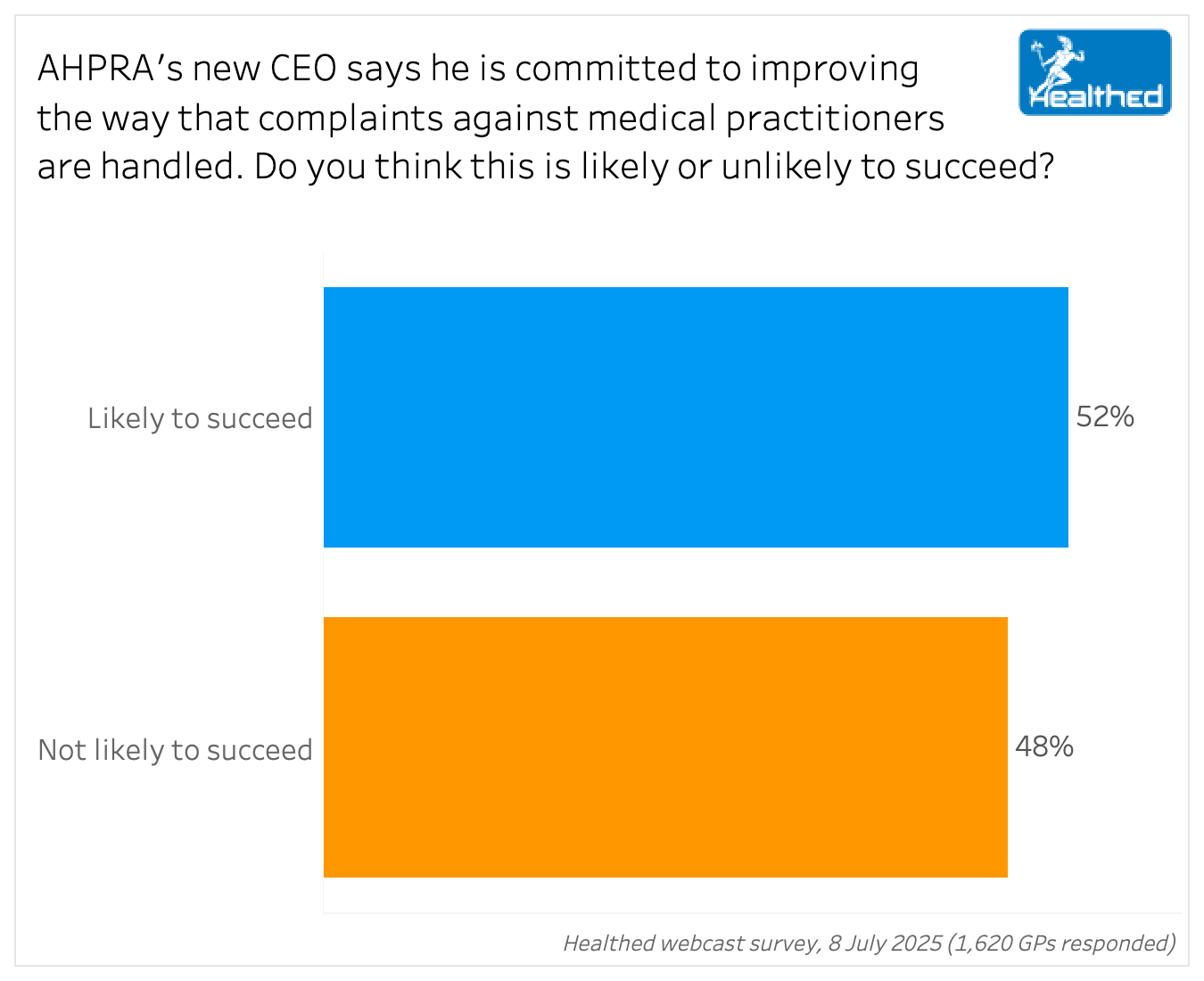
Yet just over half of GPs in the Healthed survey think AHPRA’s CEO is likely to succeed in improving how complaints are managed, with many expressing hope and optimism, and a perception that he is genuinely committed to the cause.
“Sincere efforts have not been put in so far. I believe the new CEO is sincere about improving the way complaints will be handled,” one said.
Among those who are hopeful is lawyer David Gardner, a former AHPRA manager and investigator who is now director of Australian Health Professional Development which provides compliance training.
Mr Gardner notes this is the first time an AHPRA CEO has consistently stated that things need to change significantly.
“I get the sense that this CEO wants to try and get this regulator back on track,” he says. “The fact that he has picked up that significant loss of trust in a couple of months… I am cautiously optimistic that things will at least improve.”
Still, while Mr Gardner is sure the regulator will make substantial changes, he’s less confident that reforms will be effective.
“I have no doubt that there will be substantial reform. I am 100% certain about that. The thing I have doubts about is whether that will work and whether it will be effective reform.”
Mr Gardner says that health regulation schemes around the world have similar challenges and problems to ours, so there’s not an example we can model our system on.
“The issue is we’re trying to crystal ball gaze and look into the future and prevent harm, but we don’t quite know how we should do that,” Mr Gardner says.
In most cases, AHPRA won’t know if a practitioner is unsafe until they’ve caused harm to someone — and the practitioner may not think they are unsafe, Mr Gardner points out.
“And I think sometimes practitioners and members of the public don’t necessarily appreciate how hard it is to identify if this person is a risk. I remember having cases when I worked at AHPRA where I would genuinely have no idea whether or not this person was an absolute danger or completely safe and just misunderstood.”
While he agrees we need to put more work into preventing harm, he is concerned it could lead to “Minority Report” style practices.
“Which are things like,‘well, we know the cohort that is most likely to receive a complaint is male, over 50, trained outside of Australia so therefore, we’re going to regulate those people harder.’ I think that’s profoundly unfair,” he says.
Offering extra education and support to higher-risk cohorts could be fairer and more effective, he adds.
But trying to predict the future, particularly in a fair way, “is a somewhat impossible task,” Mr Gardner says.
Many survey respondents said engrained structures—including a negative attitude towards doctors—would hinder meaningful reform.
“AHPRA’S structure and ethos are all skewed against health practitioners,” one said, while another said “Red tape and entrenched bureaucracy will derail any efforts.”
Mr Gardner agrees an internal shift is needed for reforms to succeed, noting subconscious biases can influence investigative outcomes.
“Something I have absolutely seen at an investigator level, at a board member level, and at a performance assessment level particularly, is that the mindset you have is massive in terms of how you go about it. Because if you’re saying, ‘I need to work out what happened’, versus ‘I need to work out what this person did wrong,’ you are going to end up in such different places,” he says.
Performance assessors, for example, can go out thinking they need to prove what a practitioner has done wrong, rather than whether they are meeting minimum safe standards, Mr Gardner says.
“And that just means the whole investigation is tainted from that point on, because the evidence you put forward to the board is tainted.”
Most of these mindset issues are subconscious, he stresses, but they need to be picked up and changed for reform to succeed.
Paediatric urologist and paediatric general surgeon Professor Paddy Dewan is less optimistic.
Professor Dewan, who has a long history with AHPRA—both as an instigator and recipient of complaints and an outspoken proponent of reform—says AHPRA will need a paradigm shift to overcome its current level of dysfunction.
“Unless we have a sense of revolution, a complete turning on its head, then we’re not going to get change. Just because we’ve had a CEO coming in over the top of 11,000 people isn’t necessarily going to get the culture shift that we need,” he says.
Lack of accountability within the organisation is a key problem, he says, citing cases where investigating officers have hidden important information.
“And if somebody is falsely accused and they’re put through hell, and they commit suicide, who loses their job? Nobody,” Professor Dewan says.
Indeed, Mr Gardner says information has been mishandled in several cases, including one in South Australia “where the Supreme Court found an investigator had deleted parts of a file note that were positive for the practitioner in order to get an outcome the board wanted.”
Professor Dewan believes we need an independent forensic investigation into AHPRA’s complaints handling processes.
“I think they should be investigating the investigations, as the Forrester Commission did for Minister Springborg in Queensland in 2013, where two-thirds of investigations were found to be conducted inadequately,” he says.
Other surveyed GPs were doubtful a new CEO could override long-standing issues, with many citing past failures as cause to doubt current promises.
“The problems have been around since the beginning, and despite attempts made to improve them, have remained unchanged,” one GP commented.
“Experience is AHPRA will just do what they have always done,” another summarised.
This is a legitimate concern, Mr Gardner says, noting past efforts have often focused on specific issues rather than system-wide reform, or done without full support from key people within the organisation.
Since AHPRA started, it has “flip-flopped between different case management styles” to try and fix its problems, he explains.
“Meanwhile, staff have seen constant structural change. And when I was working there, a lot of that change was driven from the very top, without almost any consultation or advice sought from the people who actually did the work.”
At the same time, numerous recommendations from Senate inquiries and reports have never been implemented, as is outlined in the Dawson review, he adds.
Healthed reached out to AHPRA, but Mr Untersteiner declined to comment.
Some GPs are hopeful:
“I am hoping it will succeed, it is possible if he has good intentions; where there is a will, there is a way.”
“He is aware that there are deficiencies and recognises a need to improve.”
“He said that he is committed to improving it, I have to trust him and give him a chance of improving the system.”
“The new CEO seems to be a very balanced human determined to reform AHPRA complaints processes more humanly to make it less dreadful for doctors and their families.”
“If there is a commitment and good faith in his endeavour to change, we should give him a chance.”
“There is plenty of room for improvement, so it should be possible.”
“Surely it cannot get any worse. The only way is up.”
“He is positive, aware of issues and doing something about them.”
Others are unconvinced:
“History repeats itself. Same plane, two different wings.”
“Same old, same old. I sincerely hope I am wrong!”
“After many years in the profession, I’ve heard it all before.”
“I don’t have confidence in AHPRA in supporting and representing doctors.”
“I don’t believe AHPRA has any incentive to improve as it doesn’t directly report to anybody.”
“You are dealing with an agency that has zero concern for the wellbeing of health practitioners and only wants ‘heads on pikes’.”
“Constitutional change is hard, and this will also be politically driven by what ‘looks good’ to the public.”
“AHPRA and the Boards exist to protect the public, not the doctor or other health practitioner, so the relationship and interaction will always be adversarial.”
“Hard for one person to change an engrained system.”




Browse the latest articles from Healthed.















